PDAC2026-06-09
PDAC at ASCO 2026: The results that matter across 17 key pipeline assets
Promising outcomes, notable Failures, and early signals that will define the future PDAC treatment landscape
ASCO 2026 featured thousands of presented abstracts, with hundreds spanning pancreatic ductal adenocarcinoma (PDAC), one of oncology's most challenging to treat indications. This report distills the key pipeline findings that drug developers and investors active in the PDAC space should be aware of coming out of the conference, covering assets that demonstrated successful outcomes, those that fell short of their targets, and early signals of promising treatments.
Section 1: Promising Clinical Outcomes covers therapies that produced considerable or meaningful efficacy results, primarily in terms of objective response rates, progression-free survival, and overall survival gains for PDAC patients. Both trial outcomes and trial design rigor (e.g., phase, sample size, randomization, statistical power) were factored into the assessment of each therapy's significance.
Section 2: Notable Failures covers assets that did not perform adequately or failed to meet pre-specified endpoint targets in their respective trials. As with the successes, trial design quality, statistical rigor, sample size, and study population were considered when evaluating the magnitude of each failure.
Section 3: Early Signals to Watch covers therapies in earlier stages of development (pre-clinical through Phase 1) with promising early signals worth monitoring as they advance through the pipeline. Several notable development stage advancements and trial initiations with implications for PDAC market entry timing were also included.
This report covers the 5 promising therapies, 5 notable underperformers, and 7 early-stage assets that were found to be most relevant for understanding where the PDAC treatment market is going. Taken together, these findings can inform ongoing competitive intelligence work in the PDAC market, shaping investment theses, clinical trial strategy, pipeline development strategy, and commercial landscape assessments for this indication.
Hover over any entry to see trial details.
Phase 1
Phase 2
Phase 3
Promising Outcomes
Notable Failures
Early Signals
Section 1: Promising Clinical Outcomes
Multiple therapies at ASCO 2026 showcased promising clinical efficacy outcomes for the future of the PDAC treatment landscape. Below are the novel therapies in development with the most successful outcomes in clinical trials, and the key pipeline assets to consider when evaluating future PDAC compeititon, commercial opportunity, and evolving treatment paradigm.
This section covers daraxonrasib, which delivered a landmark phase 3 survival readout in 2L mPDAC; surufatinib + KN046, which produced a striking 71% ORR in a heavily metastatic 1L population; XNW27011, a CLDN18.2-targeted ADC showing meaningful activity in the 2L+ biomarker-selected setting; hydroxychloroquine + chlorphenesin carbamate in combination with mFOLFIRINOX with promising safety and early signals of survival benefit; and atebimetinib, a MEK inhibitor showing improved response and PFS over SOC gemcitabine/nab-paclitaxel in a phase 2a study with a phase 3 trial planned.
1. Daraxonrasib (Revolution Medicines)
Drug Names: Daraxonrasib, RMC-6236
MOA / Modality: RAS(ON) multi-selective, tri-complex inhibitor of the active, GTP-bound state of mutant and wild-type RAS
ROA: Oral
Treatment Regimen: Daraxonrasib monotherapy vs. investigator's choice SOC chemotherapy
Sponsor: Revolution Medicines
Sponsor Country: US
Trial Name / NCT ID: RASolute 302 (NCT06625320)
Trial Details: Global phase 3, dual-arm study vs. SOC chemotherapy
Target Population: 2L metastatic PDAC
Key Outcomes
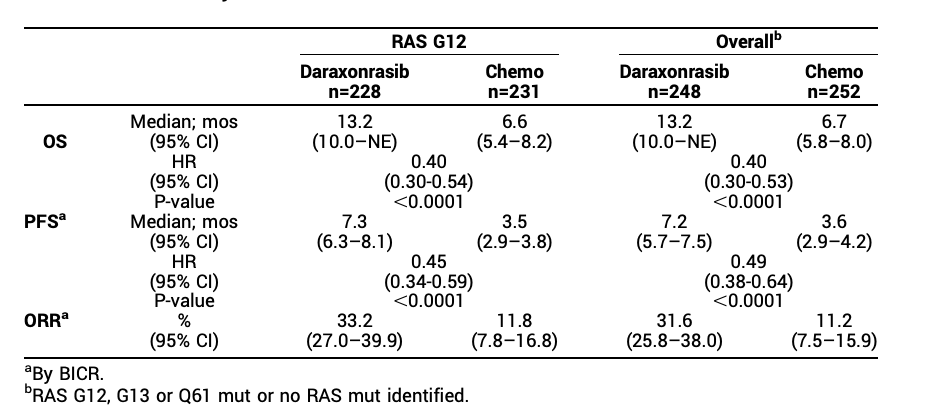
In 248 pts randomized to daraxonrasib vs. 252 to SOC chemo in 2L mPDAC (ECOG PS 0–1), both dual primary endpoints were met at data cutoff Feb 10, 2026 (median follow-up 8.5 mo). In the RAS G12 mutant population: median OS 13.2 mo (95% CI 10.0–NE) vs. 6.6 mo (95% CI 5.4–8.2), HR 0.40 (95% CI 0.30–0.54), p<0.0001; median PFS 7.3 mo (95% CI 6.3–8.1) vs. 3.5 mo (95% CI 2.9–3.8), HR 0.45 (95% CI 0.34–0.59), p<0.0001. In the overall population: median OS 13.2 mo vs. 6.7 mo, HR 0.40 (95% CI 0.30–0.53), p<0.0001; median PFS 7.2 mo vs. 3.6 mo, HR 0.49 (95% CI 0.38–0.64), p<0.0001. ORR 33.2% vs. 11.8% (RAS G12). Grade ≥3 TRAEs 43.6% (daraxonrasib) vs. 57.5% (chemo). Discontinuation due to TRAEs 1.2% vs. 11.2%.
Success Rating: Considerable
Rationale
The historical benchmark for 2L mPDAC is mOS 6–7 mo and mPFS 3–4 mo with SOC chemotherapy. Daraxonrasib approximately doubled both OS (13.2 vs. 6.6 mo) and PFS (7.3 vs. 3.5 mo) in the RAS G12 population, with an OS HR of 0.40, a magnitude of benefit rarely seen in any randomized PDAC trial. All dual primary and key secondary endpoints were met in both the RAS G12 and overall populations with p<0.0001. The abstract conclusion states: "Results support daraxonrasib as the new SOC for 2L mPDAC." The safety profile was meaningfully better than chemotherapy, with lower grade ≥3 TRAEs and a 10-fold lower discontinuation rate. Achieving these results in a second-line PDAC setting is a considerable achievement.
2. Surufatinib + KN046 (Hutchmed, Alphamab)
Drug Names: Surufatinib (HMPL-012), KN046
MOA / Modality: Surufatinib: multikinase inhibitor; KN046: bi-specific PD-L1/CTLA-4 antibody
ROA: Surufatinib: oral; KN046: IV
Treatment Regimen: Surufatinib + KN046 + SOC chemotherapy (gemcitabine and nab-paclitaxel)
Sponsor(s): Hutchmed, Alphamab
Sponsor Country: China (both)
Trial Name / NCT ID: NCT05832892
Trial Details: Single-arm, phase 1b/2
Target Population: Unresectable Advanced PDAC
Key Outcomes
In 31 treatment-naive pts with advanced PDAC (90.3% distant metastasis, 77.4% liver metastasis at baseline), ORR was 71.0% (95% CI 52.0–85.8%) including 4 CRs, 18 PRs, 6 SDs; DCR 90.3% (95% CI 74.2–98.0%). At median follow-up of 15.9 months: median PFS 8.2 mo (95% CI 6.1–NE); median OS 18.0 mo (95% CI 13.8–NE); 12-month OS rate 68.2% (95% CI 50.8–91.6%). CA199 decline ≥50% correlated with improved PFS (10.3 vs. 8.1 mo, p=0.01). Grade ≥3 TRAEs in 45.2% of pts; no treatment-related deaths.
Success Rating: Considerable
Rationale
Standard 1L gemcitabine + nab-paclitaxel yields real-world clinical ORRs in the 30–40% range, making the 71% ORR seen here a considerable outcome (De Vita et al., 2016). This is especially significant given a patient population that was predominantly metastatic with high liver metastasis burden, which typically predicts worse outcomes. The median OS of 18.0 mo is also notable but requires validation in a SOC-controlled dual-arm trial to determine net clinical benefit. This is a single-arm phase 1b/2 study with n=31, so the result is preliminary.
3. XNW27011 (Evopoint Biosciences + Astellas)
MOA / Modality: Topoisomerase inhibitor (TOP1i)-based antibody-drug conjugate targeting CLDN18.2
ROA: IV
Treatment Regimen: XNW27011 monotherapy
Sponsor(s): Evopoint Biosciences (China rights), Astellas (global rights ex-China, via licensing)
Sponsor Country: China (Evopoint), Japan (Astellas)
Trial Name / NCT ID: NCT06792435
Trial Details: Single-arm, phase 2
Target Population: 2L+ patients with CLDN18.2-positive PDAC
Key Outcomes
In 30 evaluable CLDN18.2+ PDAC pts; 37.5% had received 1 prior line; 45.8% previously treated with a TOP1 inhibitor: ORR 26.7%, DCR 83.3%, median PFS 4.1 mo, median OS 10.0 mo (median follow-up 8.1 mo). In the 1 prior line subgroup (n=13): ORR 46.2%, DCR 100%, mPFS 4.4 mo, OS not yet mature (current mOS 10.1 mo). In pts previously treated with TOP1i (n=22): mPFS 5.2 mo, mOS 10.0 mo. Grade ≥3 TRAEs 77.1%; discontinuation due to TRAEs 6.3%.
Success Rating: Moderate
Rationale
The abstract background states that median OS for PDAC pts who received ≥1 prior line of standard treatment is 6.2–7.4 months. XNW27011 achieved a median OS of 10.0 mo in this 2L+ population, including pts previously exposed to TOP1 inhibitors, suggesting activity beyond prior TOP1i exposure. The 46.2% ORR and 100% DCR in the 1L-pretreated subgroup are particularly notable. The success is rated moderate given survival gains that are meaningful but not exceptional, single-arm design only, and a high rate of grade ≥3 TRAEs (77.1%).
4. Hydroxychloroquine (HCQ) + Chlorphenesin Carbamate (CPC) (Oncocross)
MOA / Modality: HCQ: small molecule autophagy inhibitor (lysosomal acidification inhibitor); CPC: small molecule AKT-mediated epithelial-mesenchymal transition inhibitor
ROA: HCQ: oral; CPC: oral
Treatment Regimen: HCQ + CPC in combination with mFOLFIRINOX chemotherapy
Sponsor: Oncocross
Sponsor Country: South Korea
Trial Name / NCT ID: NCT05083780
Trial Details: Single-arm, phase 2
Target Population: 1L locally advanced unresectable + metastatic PDAC
Key Outcomes
Primary endpoint was safety. In 40 treated pts (73% metastatic, 27% locally advanced; median 13 cycles received): grade 3–4 neutropenia 40%, nausea 13%, anemia 10%, consistent with known mFOLFIRINOX AEs. In 39 efficacy-evaluable pts: ORR 39% (15 CR or PR), DCR 92.3% (36 pts). With a median follow-up of 33.3 mo, median PFS was 7.4 mo (95% CI 6.2–13.3); in responders, median PFS 13.6 mo (95% CI 7.4–33.8). Median OS 14.8 mo (95% CI 9.6–27.9); 20.5 mo for locally advanced, 13.9 mo for metastatic. HRQOL did not deteriorate during first 6 months.
Success Rating: Moderate
Rationale
The primary safety endpoint was met; the HCQ/CPC combination did not meaningfully worsen the mFOLFIRINOX toxicity profile. The secondary efficacy signals are positive but not substantial improvements: ORR of 39% and DCR of 92.3% are a slight improvement on mFOLFIRINOX alone, which has an ORR in the 30–40% range and DCR 70–80% (Tong et al., 2018). A median PFS of 7.4 mo is also clinically meaningful in this advanced population. Classified as moderate given the single-arm design and efficacy gains that do not substantially exceed SOC benchmarks.
5. Atebimetinib (Immuneering Corporation)
Drug Names: Atebimetinib, IMM-1-104
MOA / Modality: Small molecule deep cyclic inhibitor (DCI) of MEK
ROA: Oral
Treatment Regimen: Atebimetinib + modified gemcitabine/nab-paclitaxel (mGnP) chemotherapy
Sponsor: Immuneering Corporation
Sponsor Country: US
Trial Name / NCT ID: NCT05585320
Trial Details: Single-arm, phase 2a
Target Population: 1L advanced or metastatic PDAC
Key Outcomes
In 55 enrolled and treated pts (100% ECOG PS 0–1, median age 68, 1L advanced or metastatic PDAC), 50 were response-evaluable. Best overall responses: 21 PR, 21 SD, 7 PD, 1 NE. ORR 42%, DCR 84%. At median follow-up of 10.4 months (data cutoff Jan 7, 2026): median PFS 8.3 months; median OS was not reached, but 6- and 9-month OS rates were 88% and 79%, respectively. No grade 4 or 5 TRAEs related to atebimetinib; grade 3 TRAEs related to atebimetinib in 29% of pts. A Ph3 registrational trial of atebimetinib + mGnP vs. SOC GnP is planned to initiate mid-2026.
Success Rating: Moderate
Rationale
The authors benchmark against the MPACT trial (Von Hoff et al., 2013), which established GnP as SOC with an ORR of approximately 23% and median PFS of 5.5 months. Atebimetinib + mGnP achieved ORR of 42% and median PFS of 8.3 months, meaningful improvements in a comparably sized 1L population. The 9-month OS rate of 79% with median OS not yet reached at 10.4 months is directionally strong, though OS data remains immature. Classified as moderate success given the single-arm, non-randomized Ph2a design without a SOC control arm. The planned Ph3 registrational trial indicates the program has cleared an internal decision gate.
Section 2: PDAC Trials That Underperformed
Several therapies did not meet the necessary thresholds for meaningful efficacy in PDAC and broader pancreatic indications. A few of these are novel assets with no approved indications, while others are approved treatments used widely in other areas of oncology but demonstrating limited efficacy in pancreatic cancer.
1. BXCL701 + Pembrolizumab (BioXcel Therapeutics, Merck)
MOA / Modality: BXCL701: small molecule inhibitor of dipeptidyl peptidases 4, 8, 9 and fibroblast activation protein; Pembrolizumab: humanized IgG4 kappa monoclonal antibody, immune checkpoint inhibitor targeting the PD-1 receptor on T-cells
ROA: BXCL701: oral; Pembrolizumab: IV
Treatment Regimen: BXCL701 + pembrolizumab
Sponsor(s): BioXcel Therapeutics, Merck
Sponsor Country: US (both)
Trial Name / NCT ID: EXPEL PANC (NCT05558982)
Trial Details: Single-arm, phase 2
Target Population: 2L advanced PDAC
Key Outcomes
In 21 enrolled pts (18 evaluable) with 2L advanced PDAC: 18-week PFS rate was 22% (4/18 pts), falling below the pre-specified threshold of 7/19 pts (37%) required to trigger stage 2 of the Simon's two-stage design. Median PFS 2.3 mo (95% CI 1.6–5.3). ORR 17% (3 PRs); DCR 39%. Median OS not reached (95% CI 4.5–NR). 3 pts (14%) had PFS >6 months. One responder had MSI-H PDAC; 2 responses occurred in MSS pts. No new safety signals.
Failure Rating: Considerable
Rationale
The trial used a pre-specified Simon's two-stage design with a clear go/no-go threshold: 7 of 19 evaluable pts progression-free at 18 weeks to advance to stage 2. Only 4 of 18 evaluable pts met this threshold (22% vs. required 37%), resulting in definitive study termination at stage 1. Median PFS of 2.3 months was not appreciably distinct from historical SOC outcomes, indicating no meaningful benefit from adding BXCL701 to pembrolizumab in an unselected 2L PDAC population. The 2 MSS PDAC responders and 3 pts with PFS >6 months are noted as hypothesis-generating for biomarker-selected follow-up, but do not alter the primary failure.
2. Ibrilatazar (AbilityPharma)
Drug Names: Ibrilatazar, ABTL0812
MOA / Modality: Small molecule, dual MOA: (1) inhibiting Akt/mTORC1 pathway; (2) inducing endoplasmic reticulum stress
ROA: Oral
Treatment Regimen: Ibrilatazar + FOLFIRINOX chemotherapy vs. placebo control arm
Sponsor: AbilityPharma
Sponsor Country: Spain
Trial Name / NCT ID: PanC-ASAP (NCT04431258)
Trial Details: Dual-arm, phase 2b, placebo-controlled, 23 sites
Target Population: 1L metastatic PDAC
Key Outcomes
In 140 ITT pts, primary endpoint PFS was not met. Median PFS 9.4 mo (ibrilatazar) vs. 7.9 mo (placebo), HR 0.95 (90% CI 0.69–1.33), p=0.814. Key secondary endpoint OS not reported as significant. Pre-specified stratification revealed ECOG imbalance between arms (ECOG 0: 40% ibrilatazar vs. 54% placebo). Exploratory ECOG 0 subgroup (n=66): median PFS 11.1 vs. 6.5 mo (HR 0.60, 95% CI 0.34–1.08, p=0.089); median OS 19.3 vs. 12.0 mo (HR 0.57, 95% CI 0.31–1.05, p=0.072).
Failure Rating: Considerable
Rationale
The primary PFS endpoint was not met in the ITT population with HR 0.95 and p=0.814, indicating essentially no treatment effect. This is a properly powered, double-blind, placebo-controlled, multi-site randomized Ph2b trial, making the negative result definitive. The post-hoc ECOG 0 subgroup showing HR 0.60 for PFS and 0.57 for OS is intriguing but unplanned, driven by a baseline imbalance, and does not reach statistical significance. Classified as considerable failure because of the rigorous trial design: a randomized controlled Ph2b with 140 pts across 23 sites is a high-quality negative outcome.
3. Elraglusib (Actuate Therapeutics)
Drug Names: Elraglusib, 9-ING-41
MOA / Modality: Small molecule, glycogen synthase kinase-3β (GSK-3β) inhibitor
ROA: IV
Treatment Regimen: Arm 1: FOLFIRINOX; Arm 2: FOLFIRINOX + losartan; Arm 3: FOLFIRINOX + elraglusib; Arm 4: FOLFIRINOX + elraglusib + losartan
Sponsor: Actuate Therapeutics
Sponsor Country: US
Trial Name / NCT ID: NCT05077800
Trial Details: Multi-arm, phase 2
Target Population: 1L metastatic PDAC
Key Outcomes
In 49 pts (n=4 Arm 1, n=15 each Arms 2–4; 1L mPDAC); primary endpoint PFS: Arm 1 (FFX alone) 5.1 mo (95% CI 1.1–NR); Arm 2 (+ losartan) 5.9 mo (95% CI 1.6–9.9); Arm 3 (+ elraglusib) 6.0 mo (95% CI 1.8–9.8); Arm 4 (triple combo) 6.5 mo (95% CI 3.8–8.5). No statistical significance across arms. Median OS: Arm 1: 7.7 mo; Arm 2: 8.2 mo; Arm 3: 9.8 mo; Arm 4: 9.8 mo. Overall ORR 24.5% (12/49); SD 44.9%.
Failure Rating: Considerable
Rationale
Across all three experimental arms, median PFS and OS did not improve meaningfully or with statistical significance over the FOLFIRINOX control arm. The authors themselves note: "clinical outcomes with the novel combinations did not exceed historical standards of care." Classified as considerable failure given the dismal survival outcomes across all experimental arms.
Additional Findings
A second abstract presented post-hoc analysis from a separate elraglusib trial (open-label, phase 2) showing a more positive outlook. Elraglusib + GnP demonstrated a statistically significant OS improvement over GnP alone (mOS 10.1 vs. 7.2 months, HR 0.62, p=0.01), with 1-year survival rates of 44.1% vs. 22.3%. However, the GnP control arm performed substantially below contemporary benchmarks (7.2 vs. 9.2–9.7 months in NAPOLI-3 and PASS-01), driven by unusually high early mortality attributed to less restrictive enrollment criteria, meaning the apparent benefit may partly reflect a weak comparator rather than a true drug effect. All analyses contextualizing this control arm underperformance were post-hoc and hypothesis-generating, though the HR of 0.62 is being used to inform eligibility criteria for a planned phase 3 trial.
4. Pembrolizumab (Merck)
Drug Names: Pembrolizumab, Keytruda
MOA / Modality: Humanized IgG4 kappa monoclonal antibody, immune checkpoint inhibitor targeting the PD-1 receptor on T-cells
ROA: IV
Treatment Regimen: Pembrolizumab + olaparib; olaparib monotherapy as the control arm
Sponsor(s): Merck, NIH
Sponsor Country: US
Trial Name / NCT ID: SWOG S2001 (NCT04548752)
Trial Details: Dual-arm, phase 2
Target Population: Maintenance treatment of germline BRCA1/2-positive metastatic PDAC
Key Outcomes
73 pts enrolled, 68 eligible (vs. 88 target). Study closed early for futility after planned interim analysis. Primary endpoint PFS not improved in the combination arm (p=0.82). ORR numerically higher in the experimental arm but not statistically significant (p=0.20).

Failure Rating: Moderate
Rationale
The study was closed for futility at interim analysis with the primary endpoint PFS target (HR of 0.6, median PFS 7.0 vs. 11.7 months) not met. Authors note this as the first randomized trial of pembrolizumab and olaparib in PDAC, representing a significant blow against this combination as a viable maintenance option. The failure was rated moderate rather than considerable given that the combination builds on an already-approved core therapy (olaparib). The numerical ORR improvement and DCR signal, while not significant, suggest some biological activity that warrants translational follow-up in a biomarker-selected subgroup.
5. Binimetinib + Encorafenib (Array Biopharma / Pfizer)
Drug Names: Binimetinib (Mektovi), Encorafenib (Braftovi)
MOA / Modality: Small molecule kinase inhibitor (both)
ROA: Oral (both)
Treatment Regimen: Binimetinib + encorafenib
Sponsor: Array Biopharma (parent company: Pfizer)
Sponsor Country: US
Trial Name / NCT ID: NCT04390243
Trial Details: Two-stage, single-arm, phase 2
Target Population: 2L+ BRAF V600E mutation-positive pancreatic cancer
Key Outcomes
In 6 evaluable pts with BRAF V600E-mutant pancreatic cancer (≥2L; 1 of 7 pre-registered pts excluded for ineligibility): ORR at 24 weeks 33.3% (2/6 pts), falling below the pre-specified 40% threshold required to advance to stage 2. Overall ORR 50% (3/6 pts). Median PFS 7.1 mo, median OS 15.0 mo, median duration of response 9.9 mo, median time to response 3.9 mo. 50% of pts experienced at least one grade ≥3 AE (anemia, thromboembolic events, acute kidney injury). Study terminated due to limited accrual.
Failure Rating: Minor
Rationale
The pre-specified go/no-go threshold of 40% ORR at 24 weeks was not met (33.3%), triggering stage 2 termination per protocol. Classified as minor failure for three reasons: first, the study enrolled only 6 evaluable patients; a single additional responder would have cleared the threshold, making the result prone to random variation. Second, the overall ORR of 50% and median OS of 15.0 mo are clinically meaningful signals in a disease where 2L+ options are extremely limited, and the authors acknowledge "meaningful antitumor activity." Third, the target mutation (BRAF V600E) is present in only 2–3% of PDAC, representing a small portion of the overall treatment market.
Section 3: Early Signals to Keep an Eye On
In addition to efficacy results from phase 2 and 3 clinical trials, ASCO 2026 featured a number of therapies with early-stage results (spanning pre-clinical through phase 1) that have the potential to shape the PDAC treatment landscape further into the future. Several notable clinical development stage advancements and newly initiated trials with important implications for market entry timing were also presented. These are the assets from ASCO 2026 worth monitoring closely as they move from the horizon toward the PDAC treatment market.
1. NP137 (NETRIS Pharma)
MOA / Modality: Anti-netrin-1 antibody
ROA: IV
Treatment Regimen: NP137 + mFOLFIRINOX
Sponsor: NETRIS Pharma
Sponsor Country: France
Trial Name / NCT ID: LAP-NET1 (NCT06203821)
Trial Details: Single-arm, phase 1b
Target Population: 1L locally advanced unresectable PDAC
Key Outcomes Worth Tracking
Well tolerated with safety as primary endpoint. PFS was 10.9 months (95% CI 10.0–15.6) and median OS was 16.4 months (95% CI 12.8–NR), which may be meaningful against SOC chemotherapy survival rates in this setting.
Rationale
NP137 demonstrates tolerable safety and survival outcomes with potential for benefit over SOC. Results are from a single-arm trial, so an SOC-controlled dual-arm study will be needed to determine the level of therapeutic benefit. The therapy has potential to improve outcomes for locally advanced patients and warrants monitoring.
2. Anetumab-Ravtansine (Bayer)
MOA / Modality: ADC composed of an IgG1 antibody targeting mesothelin (MSLN) linked to DM4, a tubulin inhibitor
ROA: IV
Treatment Regimen: Arm 1: anetumab-ravtansine + nivolumab; Arm 2: anetumab-ravtansine + nivolumab + ipilimumab; Arm 3: anetumab-ravtansine + nivolumab + gemcitabine
Sponsor: Bayer
Sponsor Country: Germany
Trial Name / NCT ID: NCT03816358
Trial Details: Multi-arm, phase 1
Target Population: 2L+ metastatic PDAC
Key Outcomes Worth Tracking
Out of n=46 patients, 1 exhibited complete response, 20 had stable disease.
Rationale
While efficacy outcomes are not substantial, achieving a complete response and high levels of stable disease in a patient population with multiple prior lines of treatment is not insignificant. The study group is working to identify biomarkers that may signal treatment response to this regimen in PDAC.
3. XP-004 (Shanghai Xinpu Biotechnology)
MOA / Modality: Personalized multi-neoantigen mRNA vaccine
ROA: Intramuscular injection
Treatment Regimen: XP-004 + toripalimab (PD-1 inhibitor)
Sponsor: Shanghai Xinpu Biotechnology
Sponsor Country: China
Trial Name / NCT ID: NCT06496373
Trial Details: Single-arm, phase 1
Target Population: Adjuvant treatment for resected pancreatic cancer patients intolerant to chemotherapy
Key Outcomes Worth Tracking
All patients remained recurrence-free with no clinical or molecular evidence of disease relapse, including no tumor-informed minimal residual disease relapse. Among 13 patients evaluable for immunogenicity, 13 (100%) developed neoantigen-specific T-cell responses; 53 of 165 neoantigens (32.1%) were immunogenic.
Rationale
The vaccine + IO combination led to meaningful prevention of disease relapse after surgery. While focused on chemo-intolerant patients, promising results for adjuvant therapy with a personalized mRNA vaccine could eventually alter the SOC for adjuvant treatment in resected pancreatic cancer patients.
4. Relacorilant (Corcept Therapeutics)
MOA / Modality: Small-molecule glucocorticoid receptor antagonist
ROA: Oral
Treatment Regimen: Relacorilant + nab-paclitaxel + gemcitabine
Sponsor: Corcept Therapeutics
Sponsor Country: US
Trial Name / NCT ID: TRIDENT (NCT07259317)
Trial Details: Single-arm, phase 2
Target Population: 1L metastatic PDAC
Key Outcomes Worth Tracking
Study primary endpoint is investigator-assessed PFS, with OS, ORR, best overall response, clinical benefit rate, and duration of response as secondary efficacy endpoints. No results yet available.
Rationale
The trial has not yet read out results, but is worth monitoring once interim data becomes available. 1L mPDAC is a key segment for novel therapeutic development and any meaningful activity here would be commercially significant.
5. NC410 (NextCure)
MOA / Modality: Dimeric fusion protein of LAIR-2 with human IgG1 Fc; competitive LAIR-1 inhibitor that remodels collagen, reduces tumor growth, enhances T cell tumor infiltration, and overcomes neutrophil-mediated T cell suppression
ROA: IV
Treatment Regimen: Arm 1: NC410 + FOLFIRINOX + nivolumab; Arm 2: NC410 + FOLFIRINOX + nivolumab + ipilimumab
Sponsor: NextCure
Sponsor Country: US
Trial Name / NCT ID: NCT06941857
Trial Details: Dual-arm, phase 2
Target Population: 1L metastatic PDAC
Key Outcomes Worth Tracking
Primary endpoint is safety, with secondary efficacy endpoints of disease control rate, objective response rate, progression-free survival, and overall survival. No results yet available.
Rationale
No study results yet, but the asset should be monitored. Promising phase 2 trial results would establish NC410 as a viable candidate in the mPDAC treatment landscape, particularly given the novel LAIR-1 inhibition mechanism targeting the collagen-rich tumor microenvironment characteristic of PDAC.
6. Nesuparib (Onconic Therapeutics / Jeil Pharmaceutical)
Drug Names: Nesuparib, JPI-547
MOA / Modality: Dual tankyrase (TNKS) and poly(ADP-ribose) polymerase (PARP) inhibitor; induces a "BRCAness" phenotype via WNT and Hippo signaling
ROA: Oral
Treatment Regimen: Arm 1: nesuparib + GemAbraxane; Arm 2: nesuparib + mFOLFIRINOX
Sponsor(s): Onconic Therapeutics (parent company: Jeil Pharmaceutical)
Sponsor Country: South Korea
Trial Name / NCT ID: NCT05257993
Trial Details: Dual-arm, phase 1b
Target Population: Locally advanced or metastatic PDAC
Key Outcomes Worth Tracking
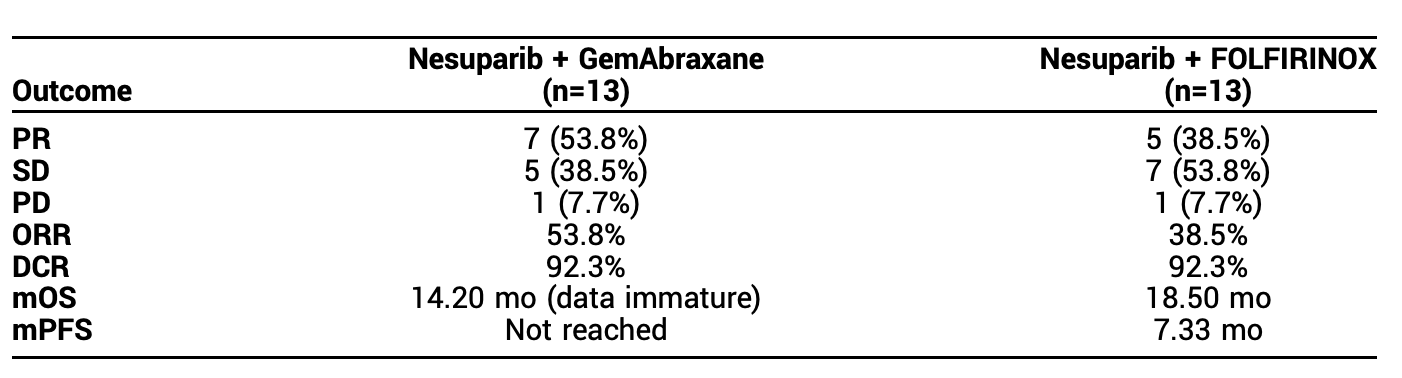
GemAbraxane arm: ORR 53.8%, DCR 92.3%, including one patient with a complete response of the target lesion and overall survival exceeding 3 years. Median PFS not reached; mOS 14.2 months (data immature, follow-up ongoing).
mFOLFIRINOX arm: ORR 38.5%, DCR 92.3%; mPFS 7.33 months, mOS 18.5 months.
Rationale
Preliminary efficacy results demonstrate survival outcomes beyond what SOC chemotherapy typically provides in this setting. The asset should be monitored as further SOC-controlled trials may validate clinical benefit, particularly given the strong DCR signal across both arms.
7. Proglumide (CCKr Therapeutics / Georgetown University)
MOA / Modality: Small molecule, cholecystokinin-B receptor (CCK-BR) antagonist
ROA: Oral
Treatment Regimen: Proglumide + gemcitabine (GEM) + nab-paclitaxel (NAB-P)
Sponsor(s): CCKr Therapeutics, Georgetown University
Sponsor Country: US
Trial Name / NCT ID: PROGEM (NCT05827055)
Trial Details: Single-arm, phase 1
Target Population: 1–2L metastatic PDAC
Key Outcomes Worth Tracking
Tumor microenvironment analysis showed decreasing fibrosis and immunosuppression while increasing T-cell infiltration. Phase 2 recommended dose was determined, with promising results justifying phase 2 trial initiation.
Rationale
While results remain limited to safety and biomarker analysis, they merit continuation of clinical evaluation. The TME remodeling data (reduced fibrosis and immunosuppression alongside increased T-cell infiltration) addresses a core challenge of PDAC biology and warrants monitoring as proglumide advances to phase 2.
References
- [1]“ASCO 2026 Late Breaking Abstract Repository” · American Society of Clinical Oncology · June 1, 2026 View source
- [2]“ASCO 2026 Gastrointestinal, Gastroesophageal, Pancreatic & Hepatobiliary Abstract Repository” · American Society of Clinical Oncology · June 1, 2026 View source
- [3]“ASCO 2026 Developmental Therapeutics — Molecularly Targeted Agents & Tumor Biology Abstract Repository” · American Society of Clinical Oncology · June 1, 2026 View source
- [4]“ASCO 2026 Developmental Therapeutics — Immunotherapy Abstract Repository” · American Society of Clinical Oncology · June 1, 2026 View source
- [5]“RASolute 302: Daraxonrasib vs. SOC Chemotherapy in 2L Metastatic PDAC (Phase 3)” · NCT06625320 · Revolution Medicines · ClinicalTrials.gov · June 1, 2026 View source
- [6]“Surufatinib + KN046 + Gemcitabine/Nab-Paclitaxel in 1L Advanced PDAC (Phase 1b/2)” · NCT05832892 · Hutchmed, Alphamab · ClinicalTrials.gov · June 1, 2026 View source
- [7]“XNW27011 (CLDN18.2 ADC) in 2L+ CLDN18.2-Positive PDAC (Phase 2)” · NCT06792435 · Evopoint Biosciences, Astellas · ClinicalTrials.gov · June 1, 2026 View source
- [8]“HCQ + CPC + mFOLFIRINOX in 1L Locally Advanced/Metastatic PDAC (Phase 2)” · NCT05083780 · Oncocross · ClinicalTrials.gov · June 1, 2026 View source
- [9]“Atebimetinib + mGnP in 1L Advanced/Metastatic PDAC (Phase 2a)” · NCT05585320 · Immuneering Corporation · ClinicalTrials.gov · June 1, 2026 View source
- [10]“EXPEL PANC: BXCL701 + Pembrolizumab in 2L Advanced PDAC (Phase 2)” · NCT05558982 · BioXcel Therapeutics, Merck · ClinicalTrials.gov · June 1, 2026 View source
- [11]“PanC-ASAP: Ibrilatazar (ABTL0812) + FOLFIRINOX vs. Placebo in 1L Metastatic PDAC (Phase 2b)” · NCT04431258 · AbilityPharma · ClinicalTrials.gov · June 1, 2026 View source
- [12]“Elraglusib ± Losartan + FOLFIRINOX in 1L Metastatic PDAC (Phase 2)” · NCT05077800 · Actuate Therapeutics · ClinicalTrials.gov · June 1, 2026 View source
- [13]“SWOG S2001: Pembrolizumab + Olaparib vs. Olaparib Maintenance in Germline BRCA1/2-Positive Metastatic PDAC (Phase 2)” · NCT04548752 · Merck, NIH / SWOG · ClinicalTrials.gov · June 1, 2026 View source
- [14]“Binimetinib + Encorafenib in 2L+ BRAF V600E-Mutant Pancreatic Cancer (Phase 2)” · NCT04390243 · Array Biopharma / Pfizer · ClinicalTrials.gov · June 1, 2026 View source
- [15]“LAP-NET1: NP137 + mFOLFIRINOX in 1L Locally Advanced Unresectable PDAC (Phase 1b)” · NCT06203821 · NETRIS Pharma · ClinicalTrials.gov · June 1, 2026 View source
- [16]“Anetumab-Ravtansine + Checkpoint Inhibitors ± Gemcitabine in 2L+ Metastatic PDAC (Phase 1)” · NCT03816358 · Bayer · ClinicalTrials.gov · June 1, 2026 View source
- [17]“XP-004 Personalized mRNA Vaccine + Toripalimab in Resected Pancreatic Cancer (Phase 1)” · NCT06496373 · Shanghai Xinpu Biotechnology · ClinicalTrials.gov · June 1, 2026 View source
- [18]“TRIDENT: Relacorilant + Nab-Paclitaxel + Gemcitabine in 1L Metastatic PDAC (Phase 2)” · NCT07259317 · Corcept Therapeutics · ClinicalTrials.gov · June 1, 2026 View source
- [19]“NC410 + FOLFIRINOX + Nivolumab ± Ipilimumab in 1L Metastatic PDAC (Phase 2)” · NCT06941857 · NextCure · ClinicalTrials.gov · June 1, 2026 View source
- [20]“Nesuparib (JPI-547) + GemAbraxane or mFOLFIRINOX in Locally Advanced/Metastatic PDAC (Phase 1b)” · NCT05257993 · Onconic Therapeutics / Jeil Pharmaceutical · ClinicalTrials.gov · June 1, 2026 View source
- [21]“PROGEM: Proglumide + Gemcitabine + Nab-Paclitaxel in 1–2L Metastatic PDAC (Phase 1)” · NCT05827055 · CCKr Therapeutics, Georgetown University · ClinicalTrials.gov · June 1, 2026 View source
- [22]“NAB-paclitaxel and gemcitabine in metastatic pancreatic ductal adenocarcinoma (PDAC): from clinical trials to clinical practice” · De Vita et al. / BMC · September 2, 2016 View source
- [23]“The benefits of modified FOLFIRINOX for advanced pancreatic cancer and its induced adverse events: a systematic review and meta-analysis” · Tong et al. / Nature Scientific Reports · June 6, 2018 View source
Abstracts Covered
- [1]Daraxonrasib, a RAS(ON) multi-selective inhibitor vs chemotherapy in previously treated metastatic pancreatic adenocarcinoma (mPDAC): Primary and final analysis from the phase 3 RASolute 302 study
- [2]Surufatinib plus KN046 and chemotherapy as first-line treatment for advanced pancreatic ductal adenocarcinoma: Updated results and biomarker analysis from a phase 1b/2 trial
- [3]Efficacy and safety of XNW27011, a Claudin-18.2 targeted (CLDN18.2) ADC, in advanced pancreatic ductal adenocarcinoma: A phase 2 study
- [4]Multicenter phase 2 study of hydroxychloroquine (HCQ) and chlorphenesin carbamate (CPC) in combination with mFOLFIRINOX in patients with advanced pancreatic adenocarcinoma (PDAC)
- [5]Results from a phase 2a study of atebimetinib in combination with mGnP in advanced or metastatic pancreatic cancer
- [6]BXCL701 plus pembrolizumab in second-line advanced pancreatic ductal adenocarcinoma: Final outcomes of the EXPEL PANC trial
- [7]Phase IIb randomized trial of FOLFIRINOX plus ibrilatazar (ABTL0812) versus placebo as first-line treatment in metastatic pancreatic cancer: An analysis from the PanC-ASAP study
- [8]A phase II study of FOLFIRINOX (FFX) combined with the glycogen synthase kinase-3beta (GSK-3β) inhibitor elraglusib (ELRA) and the transforming growth factor beta (TGFβ) inhibitor losartan (LOS) in patients with untreated metastatic pancreatic ductal adenocarcinoma (mPDAC)
- [9]Post-hoc efficacy and biomarker analysis of elraglusib plus gemcitabine/nab-paclitaxel versus chemotherapy alone in metastatic pancreatic ductal adenocarcinoma
- [10]Randomized phase II trial of olaparib and pembrolizumab vs olaparib alone as maintenance therapy in metastatic pancreatic cancer patients with germline BRCA1 or BRCA2 mutations: SWOG S2001
- [11]A phase II trial of binimetinib in combination with encorafenib in patients with pancreatic malignancies and a somatic BRAF V600E mutation
- [12]LAP-NET1: Results of a phase 1b evaluating NP137, an inhibitor of the epithelial-to-mesenchymal transition, in combination with mFOLFIRINOX for the first-line treatment of locally advanced pancreatic ductal adenocarcinoma
- [13]Final results and preliminary correlative analysis of a phase I study of anetumab ravtansine in combination with checkpoint inhibitors and gemcitabine in mesothelin-positive advanced pancreatic adenocarcinoma (NCI10208)
- [14]An investigator-initiated phase I study evaluating the safety, tolerability, and preliminary efficacy of a personalized neoantigen mRNA vaccine (XP-004) combined with PD-1 inhibitor as adjuvant therapy in resected pancreatic cancer patients intolerant to chemotherapy
- [15]TRIDENT: A phase 2 study of relacorilant plus nab-paclitaxel and gemcitabine in patients with previously untreated metastatic pancreatic ductal adenocarcinoma
- [16]Phase II study of NC410 and FOLFIRINOX in combination with nivolumab with or without ipilimumab in patients with treatment-naive metastatic pancreatic cancer
- [17]Safety and efficacy of nesuparib (JPI-547) with gemcitabine-nab-paclitaxel (GemAbraxane) or modified FOLFIRINOX (mFOLFIRINOX) in patients with locally advanced or metastatic PDAC: Results from an ongoing phase Ib/II study
- [18]Proglumide, gemcitabine (GEM), and nab-paclitaxel (NAB-P) in patients with pancreatic ductal adenocarcinoma (PDAC): Results of the phase 1 PROGEM trial
Read the full report
Enter your details below to access the complete analysis.
Didn't find the data you were looking for?
Let us know what we missed.